What Are the Most Effective Treatments for Melasma?
By Teresa Alasio, MD | Intentional Self Aesthetics, New Canaan, CT
Melasma is treatable, but it requires a more nuanced approach than most pigmentation conditions. The wrong treatment can worsen it. The right protocol, sustained consistently, produces meaningful and lasting improvement.
The foundation: sun protection above everything else:
No melasma treatment works without rigorous, daily sun protection. UV exposure is the primary trigger for melanocyte overactivation, and without consistent SPF 50, broad-spectrum sunscreen applied every morning and reapplied throughout the day, any improvement achieved in the treatment room will fade within weeks. This is non-negotiable and it is where every melasma protocol begins.
Topical prescription treatments:
Prescription-strength topical agents are the cornerstone of melasma treatment. The most established is hydroquinone, a melanocyte-inhibiting agent that reduces pigment production when used under physician supervision. Triple combination creams, containing hydroquinone, a retinoid, and a mild corticosteroid, are among the most clinically studied approaches. Tranexamic acid, azelaic acid, and kojic acid are additional options with meaningful evidence bases, particularly for patients who cannot use hydroquinone long-term.
I prescribe topical protocols individualized to each patient’s skin type, Fitzpatrick phototype, and the depth and pattern of their melasma.
In-office treatments:
Chemical peels, particularly lower-strength options appropriate for the patient’s skin type, can accelerate the clearance of superficial pigmentation. The SkinMedica peels I offer can be incorporated carefully into a melasma treatment plan for appropriate candidates.
BBL and laser treatments require significant caution with melasma. Heat-based treatments can paradoxically worsen melasma if not carefully managed. Any use of energy-based treatments in a melasma patient is done conservatively, with appropriate pre-treatment and post-treatment protocols, and after careful evaluation of skin type and melasma depth.
The depth question:
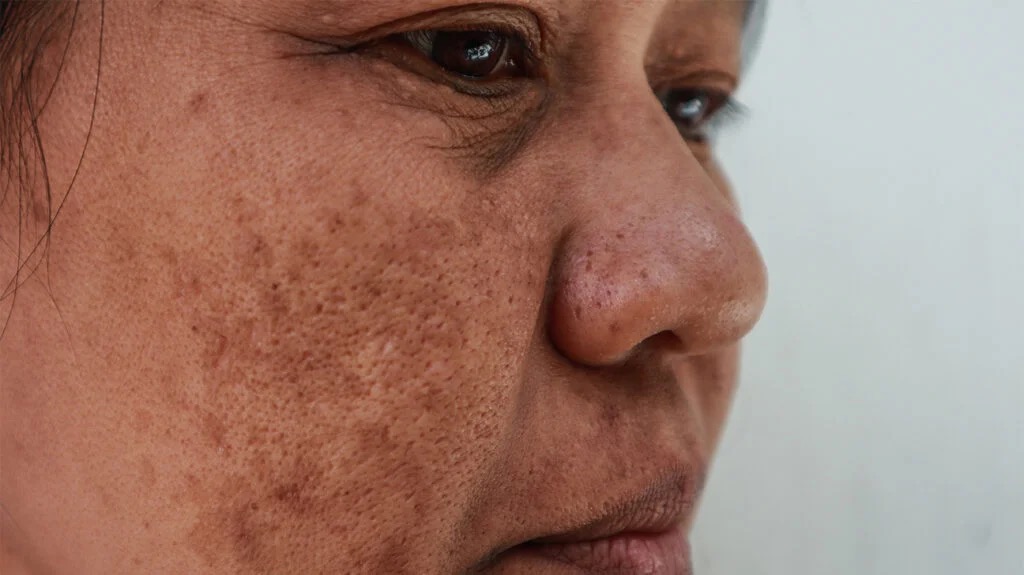
Melasma can be epidermal (in the outer skin layer), dermal (deeper), or mixed. Epidermal melasma responds better to topical treatments and peels. Dermal melasma is more difficult to treat and requires patience. A Wood’s lamp or skin analysis can help assess the depth and guide the approach.
Managing expectations:
Melasma is a chronic condition. It can be significantly improved, often to the point where it is not visible in daily life. But it is not cured. Sun protection and maintenance are lifelong commitments. Patients who understand this from the beginning have the best long-term outcomes.
Ready to start a physician-guided melasma treatment plan? Request a consultation with Dr. Alasio.
Teresa Alasio, MD is a board-certified physician in Pathology, Cytopathology, and Aesthetics and the founder of Intentional Self Aesthetics at 23 Vitti Street, New Canaan, CT.


